Case History
The patient is a 32 years old female normotensive, non diabetic, para 2, presented with chief complaints of lump in her right breast 15 days back on March 8 2020
No history of nipple discharge was present.
History of loss of weight was present.
FNAC was done on 4th march 2020 which revealed Proliferative breast disease with mild or moderate atypia.
She does not have any family history of carcinoma breast/ovary.
She underwent right breast lumpectomy on 9th March 2020, which was done under general anaesthesia in which large lump of 3cmx3cm was dissected.
HPE (S -2512/20) shows Invasive ductal carcinoma (Block review of lung)
FNAC (C- 3403/20) Consistent with duct carcinoma was investigated further.
Mammogram breast was done on 06/04/2020 which shows evidence of multiple clusters of regional premorphic calcifications in upper outer quadrant of right breast.
Increased density seen in right breast lower outer quadrant with mild orchitural distortion.
Hence BIRADS VI was classified.
PET CT scan was done on 19/03/2020 which shows Mildly metabolically active irregular hypodense area in upper inner quadrant of right breast. Mild nodularity in the lower outer quadrant of right breast.
MRI Breast was done on 06/04/2020 shows Enhancing irregular mass measuring 1.2 x 0.6 x 1.2 cm in its largest dimensions showing heterogenous enhancement non mass enhancement anteriorly,
A subcentimeter mucinous cyst at 1’o clock axis mid depth - BIRADS V and lower inner BIRADS V.
USG breast was also done on 06/04/2020 which reveals Ill defined hyperechoic region suggestive of post operative changes measuring 4.4 cm x 1.8 cm at 1’o clock position, 9 cm from nipple.
IAlso ill defined focus of dense glandular parenchyma with microcalcification measuring 1.9 cm x 0.8 cm.
Hence BIRADS VI was classified.
Dumble shaped cyst with tiny microcalcification is seen in right breast 11-12’o clock position. BIRADS IV
Patient then underwent Right MRM + Right LD flap reconstruction.
She was then discharged and received 6 cycles of TCH and 12 cycles of H protocol.
Further she developed recurrent disease with lung metastasis,
Repeat biopsy was suggestive of ER-ve, PR-ve, Her2 3+ve
Post 3 cycles of chemotherapy there was marginal increase in lung lesion
therefore plan was to give 2 more cycles and then repeat PET CT scan.
Post 5 cycles, PET CT suggestive of progressive disease.
Now plan of treatment changed to Eleftha + Vinorelbine + Lapatinib.
Post 3 cycles, PET CT suggestive of good response in lungs but with New Brain Lesion.
She received WBRT for Brain mets.
Post 6 cycles she had again progression in lungs.
Now started on Capecitabine with Eleftha.
PET CT scan was done on 18/08/2023 is suggestive of “Complete Metabolic Response” to the treatment
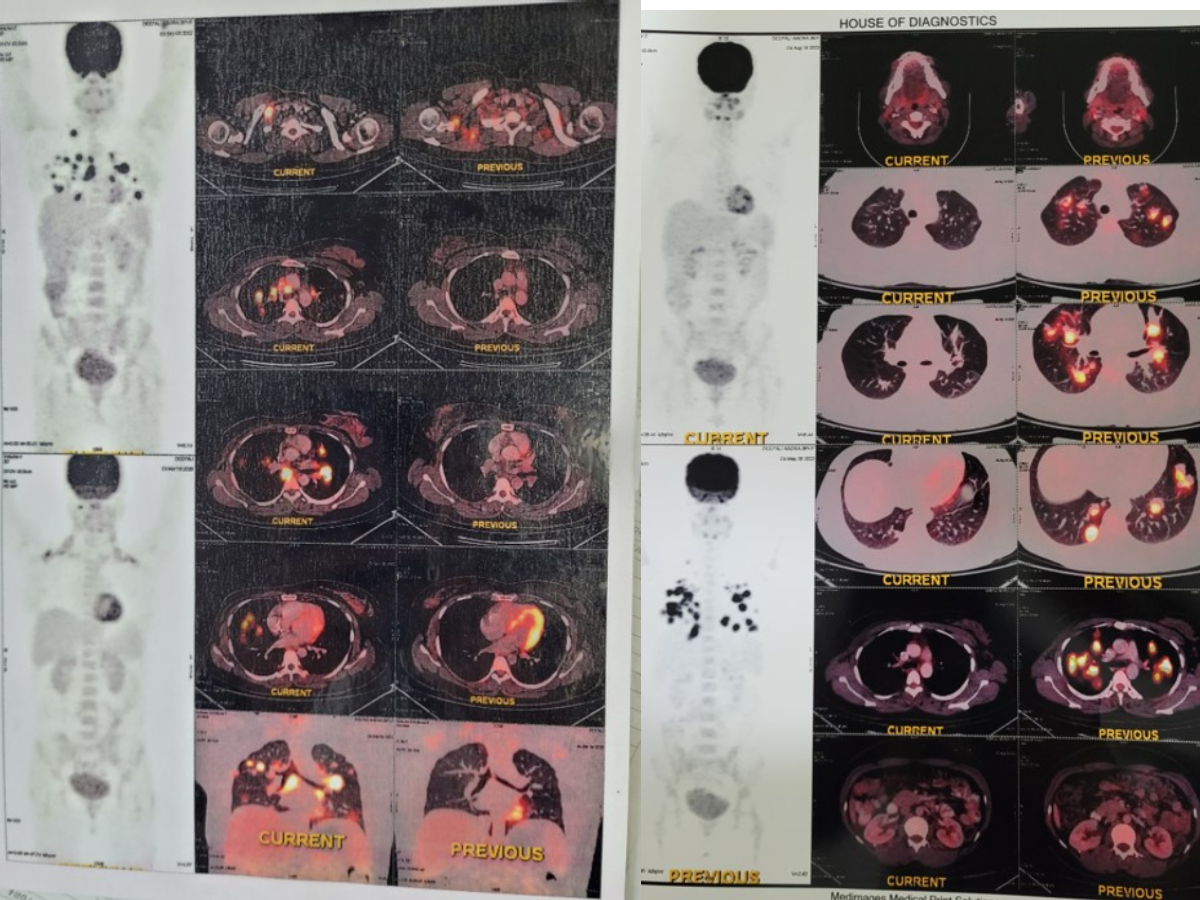
Comparision of Initial and recent PET CT scan is as follows.
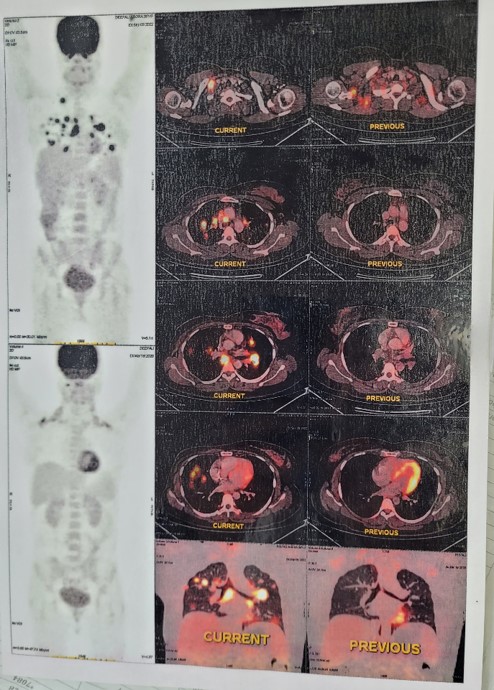
PET CT scan initially done, showing comparison of 19/03/2020 and 05/09/2020
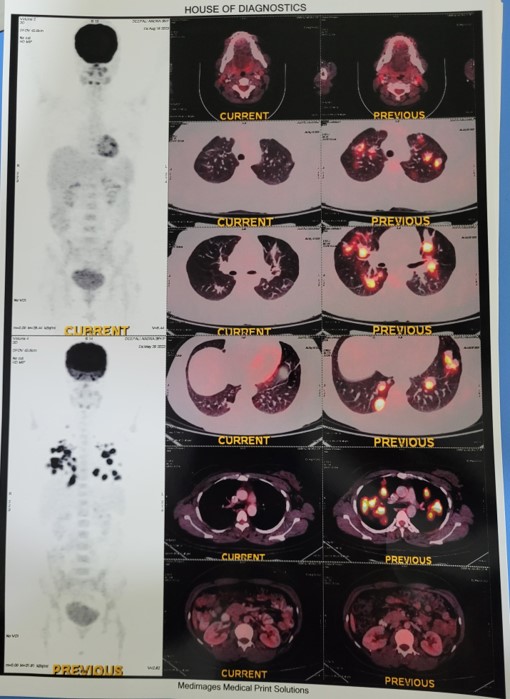
Latest PET CT scan done on 19/08/2023, showing “Complete Metabolic Response” to disease.